how-to guide
Ultrasound Guided Injections for Knee Pain: A 2026 Guide

Table of Contents
- What Are Ultrasound Guided Injections for Knee Pain?
- Step-by-Step: The Ultrasound Guided Procedure
- Joint Injection Accuracy: Ultrasound vs. Landmark-Guided Techniques
- Hyaluronic Acid Knee Injection and Alternative Injectables
Ultrasound Guided Injections for Knee Pain: A 2026 Guide
Last Updated: July 16, 2026
What Are Ultrasound Guided Injections for Knee Pain?
Ultrasound guided injections deliver therapeutic agents directly into the knee joint using real-time imaging. Unlike landmark-guided injections that rely on anatomical landmarks alone, ultrasound guidance visualizes the needle in real time, ensuring accurate placement. This precision transforms knee pain management from trial-and-error into a reproducible, evidence-based intervention.
The procedure combines musculoskeletal ultrasound imaging with targeted injection therapy. Clinicians see the needle trajectory, identify joint effusion, locate the suprapatellar recess, and confirm needle tip position before medication delivery. This diagnostic clarity allows simultaneous assessment of soft tissue integrity, synovial inflammation, and structural abnormalities, informing treatment selection between corticosteroid injections, hyaluronic acid viscosupplementation, or newer options like Arthrosamid.
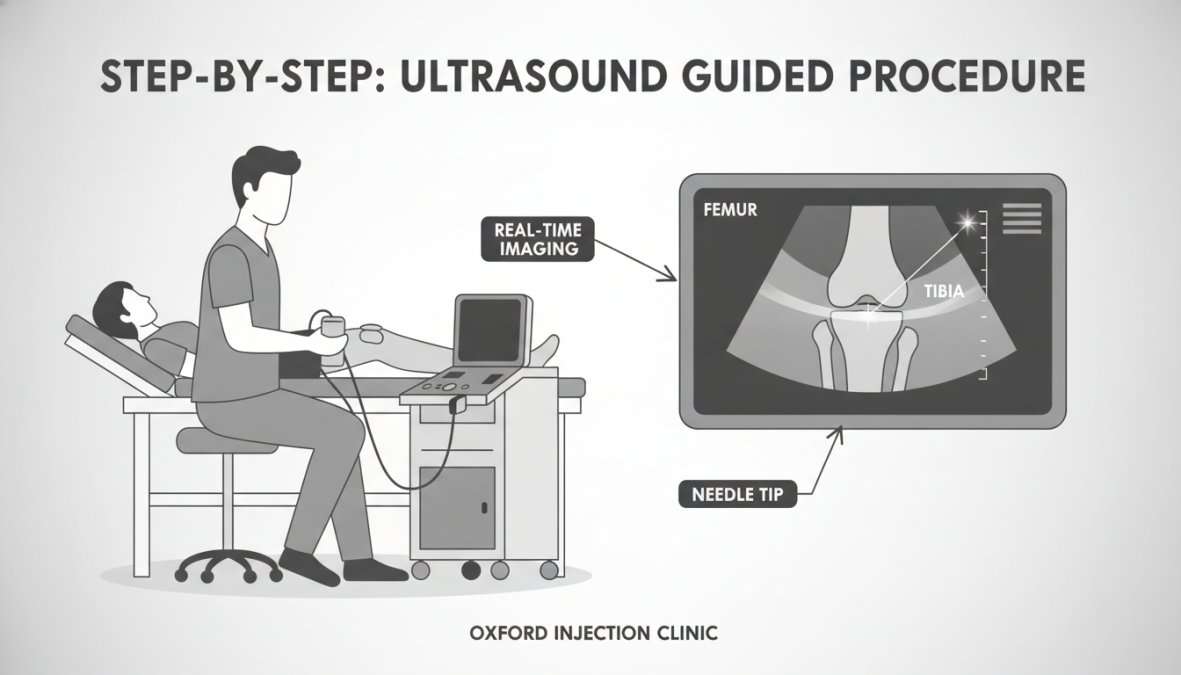
Step-by-Step: The Ultrasound Guided Procedure
Before Your Appointment: Preparation and What to Expect
Arrive 10-15 minutes early to complete consent forms. Wear loose clothing that allows easy knee access, shorts or pants that roll up above the knee are ideal. Fasting is not required, though eating a light meal 1-2 hours before helps if you're anxious about needles.
If you take anticoagulants such as warfarin or direct oral anticoagulants, discuss this with your clinician at least one week before your appointment. Some practitioners recommend temporary adjustment; others proceed without modification depending on your bleeding risk. Bring a list of all medications, supplements, and known allergies, particularly to local anesthetics or iodine-based antiseptics.
Arrange transportation home if possible, particularly if you feel lightheaded afterward. While most patients drive safely, having support available allows you to rest immediately post-procedure.
The Procedure: Real-Time Visualization and Needle Placement
You'll be positioned supine or semi-reclined with your knee slightly bent, relaxing the quadriceps and opening the joint space. Ultrasound gel is applied to conduct sound waves, and the transducer visualizes the suprapatellar recess or medial joint line depending on your anatomy.
Your skin is cleaned with an antiseptic solution and allowed to dry completely. A small amount of local anesthetic (usually 1% lidocaine) is injected into the skin, causing a brief sting lasting 5-10 seconds. The injection needle, typically 25-27 gauge, is then advanced under continuous ultrasound visualization. You'll see the needle tip on the ultrasound screen moving toward the joint. Most patients report minimal pain; the ultrasound guidance optimizes the pathway before insertion begins.
Once the needle tip reaches the joint space, confirmed by seeing it breach the joint capsule on ultrasound, the clinician injects saline to confirm placement. The therapeutic agent is then slowly injected over 30-60 seconds. The entire process typically takes 5-10 minutes. After medication delivery, the needle is withdrawn and the injection site is covered with a bandage. You'll rest for 10-15 minutes while staff monitor for adverse reactions.
Immediate Post-Procedure: The Critical First 48 Hours
Avoid strenuous activity, heavy lifting (anything over 10 pounds), or high-impact exercise such as running or jumping for 48 hours. Light walking at a comfortable pace is encouraged and beneficial, it promotes circulation and prevents stiffness.
Apply ice wrapped in a thin cloth for 15-20 minutes several times daily in the first 24 hours to reduce swelling. After 48 hours, heat may provide additional comfort. Mild post-injection soreness or fullness lasting 24-48 hours is normal. Over-the-counter acetaminophen or ibuprofen can manage discomfort, though some clinicians recommend avoiding NSAIDs for the first 48 hours to allow natural inflammatory processes to support healing.
A small percentage of patients experience a post-injection flare, temporary increased pain lasting 1-3 days before improvement begins. This is manageable with ice, rest, and pain relief, and does not indicate treatment failure.
Week 1-2: Gentle Movement and Early Rehabilitation
Beginning 3-5 days after injection, commence gentle movement and basic physiotherapy. Walk at a comfortable pace for 20-30 minutes daily. Perform gentle range-of-motion exercises: slow knee bends, straight-leg raises, and ankle circles. Most patients notice initial pain relief within 48-72 hours, with progressive improvement over 2-4 weeks. Full therapeutic benefit often develops over 8-12 weeks with consistent physiotherapy participation.
Joint Injection Accuracy: Ultrasound vs. Landmark-Guided Techniques
Landmark-guided techniques rely on palpable anatomical landmarks to estimate needle position. While experienced clinicians achieve reasonable success, accuracy depends heavily on practitioner skill and patient anatomy. Ultrasound guidance eliminates guesswork by providing real-time visualization, especially critical in patients with difficult anatomy, obesity, previous surgery, or joint effusion.
Research demonstrates ultrasound-guided techniques achieve higher first-attempt success rates. According to American Academy of Orthopaedic Surgeons clinical guidance, ultrasound-guided knee injections show success rates exceeding 95%, compared to 70-85% for landmark-guided approaches. This translates to fewer repeat procedures, faster symptom relief, and better patient satisfaction.
| Technique | Accuracy Rate | Visualization | Best For | Repeat Rate |
|---|---|---|---|---|
| Ultrasound-guided | 95%+ | Real-time needle visualization | All patients, especially complex anatomy | <5% |
| Landmark-guided | 70-85% | Anatomical landmarks only | Experienced clinicians, simple anatomy | 15-30% |
Hyaluronic Acid Knee Injection and Alternative Injectables
Hyaluronic acid injections restore joint lubrication by mimicking the body's own synovial fluid. Osteoarthritis depletes natural hyaluronic acid content, reducing lubrication and increasing friction. Hyaluronic acid injection replenishes this protective layer, reducing pain and improving mobility. Most patients receive 3-5 injections spaced one week apart, with benefits lasting 6-12 months.
Corticosteroid injections provide rapid anti-inflammatory relief, ideal for acute flare-ups or severe inflammation. These work within days and provide 4-12 weeks of pain reduction. The trade-off: repeated steroid injections carry cumulative risks, so most clinicians limit them to 3-4 per year per joint.
Arthrosamid injections represent a newer approach. This cross-linked hyaluronic acid polymer provides longer-lasting joint lubrication than standard hyaluronic acid. Arthrosamid typically requires only a single procedure, with benefits lasting 12+ months, though individual results vary.
Platelet-rich plasma (PRP) injections harness growth factors from the patient's own blood to stimulate tissue repair. While promising for early-stage osteoarthritis, PRP requires blood draw and processing time, adding cost and complexity. Results are less consistent than hyaluronic acid, and insurance rarely covers PRP for knee pain.
| Injectable Type | Onset Time | Duration | Best For | Repeat Schedule |
|---|---|---|---|---|
| Hyaluronic Acid | 3-7 days | 6-12 months | Moderate OA, chronic pain | Every 6-12 months |
| Corticosteroid | 24-48 hours | 4-12 weeks | Acute flares, severe inflammation | 3-4 times yearly max |
| Arthrosamid | 2-4 weeks | 12+ months | Long-term lubrication, OA progression | Single injection or annual |
| PRP | 2-6 weeks | 6-12 months | Early OA, cartilage damage | Every 6-12 months |
A consultant-led ultrasound MSK diagnostic assessment identifies which injectable best matches your pathology. For example, a patient with significant joint effusion and inflammation might benefit from an initial corticosteroid injection followed by hyaluronic acid maintenance.
Safety and Clinical Efficacy in Musculoskeletal Practice
Safety Profile and Adverse Effects
Ultrasound guided injections carry an excellent safety profile when performed by trained practitioners in sterile settings. Real-time visualization eliminates the risk of injecting into surrounding soft tissue, blood vessels, or nerves. Infection rates fall below 0.1% when proper sterile technique is followed.
Common side effects are mild and temporary. Post-injection soreness lasting 24-48 hours is most frequent, reflecting the body's response to injection and mechanical joint capsule distension. Swelling typically resolves within days. A small percentage experience a post-injection flare, temporary increased pain lasting 1-3 days, before therapeutic benefit begins. This is manageable with ice, rest, and over-the-counter pain relief.
Serious complications are rare. Joint infection occurs in fewer than 1 in 1,000 procedures with proper sterile technique. Allergic reactions to injected substances are uncommon but possible. Nerve or blood vessel injury is exceptionally rare with ultrasound guidance. Patients on anticoagulants may experience slightly increased bruising but not serious bleeding; most clinicians do not require discontinuation.
Clinical Efficacy and Evidence Base
Ultrasound-guided knee injections achieve pain reduction in 80-90% of patients with osteoarthritis. Functional improvement, increased walking distance, improved stair climbing, reduced medication dependence, follows in most responders. When the needle reaches the correct target, the therapeutic agent works as intended. When landmark-guided injections miss the joint space (occurring in 15-30% of cases), even excellent medications fail because the medication never reaches the intended site.
Duration of benefit varies by injectable:
-
Hyaluronic acid injections typically provide pain relief lasting 6-12 months, with peak benefit 4-8 weeks after injection. A series of 3-5 injections spaced one week apart is standard.
-
Corticosteroid injections provide rapid relief within 24-48 hours, ideal for acute flare-ups. Benefits typically last 4-12 weeks. Most clinicians limit them to 3-4 per year per joint.
-
Arthrosamid injections are designed for longer-lasting benefit. Early clinical evidence suggests pain relief lasting 12+ months from a single injection.
-
Platelet-rich plasma (PRP) injections show promise for early-stage osteoarthritis, with benefits lasting 6-12 months, though results are less consistent than hyaluronic acid.
Integration of physical therapy with injection therapy amplifies results substantially. An ultrasound-guided injection reduces pain and inflammation, creating a window for rehabilitation. Structured physiotherapy during this window rebuilds strength, restores mobility, and prevents future flare-ups. Clinics combining injections with evidence-based physiotherapy see superior long-term outcomes, with some studies showing 20-30% greater functional improvement when therapy is included.
Cost, Insurance Coverage, and Out-of-Pocket Expectations
Private Practice Costs (Self-Pay):
Ultrasound-guided knee injections typically range from £300-£800 per procedure, depending on the injectable and clinician experience. This usually includes the ultrasound MSK diagnostic scan, injection procedure, and basic post-injection guidance. Additional physiotherapy sessions are billed separately, typically £50-£150 per session.
Breakdown by injectable:
-
Hyaluronic acid injections: £300-£500 per injection. A standard course of 3-5 injections costs £900-£2,500. Some clinics offer package pricing, reducing per-injection cost by 10-20%.
-
Corticosteroid injections: £250-£400 per injection. Among the least expensive options.
-
Arthrosamid injections: £600-£800 per injection. Because only one injection is typically required, total cost is comparable to a full hyaluronic acid course, but extended duration (12+ months) often makes it cost-effective over time.
-
PRP injections: £800-£1,500 per injection. Higher cost reflects blood draw, processing, and specialized equipment. Most private insurance does not cover PRP.
NHS Coverage:
NHS coverage varies significantly by region and clinical commissioning group. Some areas fund ultrasound-guided hyaluronic acid injections for patients with confirmed osteoarthritis who failed conservative management. Others restrict coverage to corticosteroid injections only. Arthrosamid and PRP are rarely funded on the NHS.
To determine NHS eligibility, contact your GP or local rheumatology or orthopedic clinic. You'll typically need confirmed diagnosis of osteoarthritis, evidence of failed conservative management (physiotherapy, NSAIDs, weight management attempted for 3+ months), GP referral, and consultant assessment. Waiting times vary from 6-16 weeks depending on region and clinic capacity.
Private Insurance Coverage:
Most comprehensive private policies cover ultrasound-guided hyaluronic acid injections for osteoarthritis, typically with a co-payment or deductible. Corticosteroid injections are usually covered. Arthrosamid and PRP coverage is less common and varies by insurer.
Before scheduling, contact your insurer to confirm coverage for your specific injectable, determine your co-payment, verify in-network status, and obtain pre-authorization if required. This process typically takes 5-10 business days.
Physiotherapy Costs:
Private physiotherapy typically costs £50-£150 per session. A comprehensive post-injection rehabilitation program usually requires 8-12 sessions over 8-12 weeks, totaling £400-£1,800. Some private insurance policies cover physiotherapy with similar co-payments; NHS physiotherapy is free but often has longer waiting times.
Cost-Effectiveness Considerations:
A single successful ultrasound-guided injection that delays or prevents knee replacement surgery saves tens of thousands of pounds in surgical costs, hospital stays, and rehabilitation. Even paying privately, injection costs are typically a fraction of knee replacement surgery (£15,000-£30,000 in private practice). Successful pain relief often reduces reliance on daily pain medications, which carry their own costs and side effects.
Maximizing Value:
-
Confirm diagnosis first: Ensure imaging confirmation (X-ray or MRI) of osteoarthritis or other pathology.
-
Commit to physiotherapy: Injection-plus-therapy produces superior outcomes compared to injection alone.
-
Ask about package pricing: Private clinics often offer discounts for full injection courses.
-
Explore insurance options: Verify coverage before paying out-of-pocket. Pre-authorization may save hundreds of pounds.
-
Consider long-acting options: If cost is a concern, Arthrosamid's single-injection protocol and extended duration may offer better long-term value than repeated hyaluronic acid injections.
Indications for Knee Pain Management and Patient Selection
Ultrasound guided injections address many knee conditions, from osteoarthritis to post-operative inflammation. The ideal candidate has symptomatic knee pain unresponsive to conservative measures: rest, ice, anti-inflammatory medications, and basic physiotherapy.
Osteoarthritis is the most common indication. Patients with confirmed OA on imaging who experience pain limiting daily activity are excellent candidates. Injections work particularly well for those not yet ready for surgery, seeking to delay surgical intervention, or wishing to avoid long-term oral pain medication dependence.
Post-operative patients benefit significantly. After arthroscopy, meniscectomy, or other knee procedures, residual inflammation and pain are common. Targeted injections reduce post-operative swelling, accelerate recovery, and support rehabilitation.
Acute injuries, meniscal tears, ligament sprains, or traumatic effusion respond well to ultrasound-guided injections combined with physiotherapy. The ultrasound MSK diagnostic scan identifies the specific injury pattern, and the injection addresses inflammation while healing progresses.
Contraindications are limited. Active infection at the injection site, systemic infection, or uncontrolled bleeding disorders require caution. Allergy to any injectable component is an absolute contraindication.
A detailed consultation determines suitability. History, physical examination, and ultrasound imaging reveal the actual pathology driving your pain. Some patients discover pain originates elsewhere, hip pathology referred to the knee, for example, requiring different treatment. This diagnostic clarity prevents wasted procedures and directs you toward the most helpful intervention.
Post-Injection Recovery and Physical Therapy Integration
Recovery after an ultrasound-guided injection is straightforward, but the first 48 hours matter significantly. Avoid strenuous activity, heavy lifting, or high-impact exercise for at least 24-48 hours. Gentle movement, however, should begin almost immediately. Walking at a comfortable pace, light stretching, and basic range-of-motion exercises prevent stiffness and promote healing.
Ice application in the first 24 hours reduces swelling. Apply ice for 15-20 minutes several times daily if you experience post-injection discomfort. After 48 hours, heat may provide additional comfort.
Physical therapy integration is where recovery accelerates. A structured rehabilitation program beginning 3-5 days after injection targets strength deficits, restores range of motion, and builds muscular support that protects your knee long-term. The injection reduces pain and inflammation; therapy rebuilds function. This combination produces superior outcomes compared to injection alone.
A typical post-injection rehabilitation pathway includes:
- Week 1-2: Gentle range-of-motion exercises, isometric strengthening, proprioceptive training
- Week 3-4: Progressive resistance exercises, functional movement patterns, walking and stair training
- Week 5-8: Advanced strengthening, return to activity-specific training, ongoing maintenance
Most patients notice meaningful improvement within 2-4 weeks and maximum benefit by 8-12 weeks. This timeline assumes consistent physiotherapy participation; sporadic therapy delays recovery and reduces overall benefit.
The goal is to restore not just pain relief, but genuine functional capacity. A successful outcome means you can walk without pain, climb stairs without limitation, and return to activities that matter to you.
Knee pain from osteoarthritis or injury doesn't have to limit your life. Ultrasound guided injections for knee pain, combined with targeted physiotherapy, address both immediate pain and long-term function. Oxford Injection Clinic specializes in consultant-led ultrasound MSK diagnostic assessment and precision-guided injections, including hyaluronic acid, corticosteroid, and Arthrosamid options. With over 20 years of NHS and private experience, the clinic's personalized approach helps patients avoid or delay surgery while rebuilding genuine knee function. Book your consultation with Oxford Injection Clinic today and discover how precision medicine can transform your recovery.
Frequently Asked Questions
What is an ultrasound guided injection for knee pain?
An ultrasound guided injection uses high-frequency sound waves to visualize the knee joint in real-time, allowing precise needle placement directly into the joint space or affected soft tissue. Unlike landmark-guided or blind injections that rely on anatomical landmarks alone, ultrasound guided injections provide live imaging to ensure accurate medication delivery, whether corticosteroids, hyaluronic acid, Arthrosamid, or other therapeutics, directly to the source of pain, improving clinical efficacy and patient outcomes.
How accurate are ultrasound-guided knee injections compared to blind injections?
Ultrasound guided injections offer significantly higher needle accuracy than blind or landmark-guided techniques. Real-time imaging allows clinicians to visualize the joint space, synovial fluid, joint effusion, and soft tissue structures, ensuring the needle reaches the intended target. This precision reduces missed injections, minimizes adverse effects, and improves therapeutic outcomes, particularly important for osteoarthritis and chronic knee pain where accurate intra-articular placement is essential for pain relief.
What types of injectables are used in ultrasound-guided knee injections?
Common injectables include corticosteroids for rapid inflammation reduction, hyaluronic acid (viscosupplementation) for joint lubrication and cushioning, Arthrosamid for long-term osteoarthritis relief, and platelet-rich plasma (PRP) for tissue regeneration. Your consultant will recommend the best option based on your diagnosis, severity of knee osteoarthritis, and individual goals. MSK ultrasound diagnostic scanning helps identify which injectable and approach will deliver the best outcomes for your specific condition.
What should I expect during recovery after an ultrasound-guided knee injection?
Most patients experience minimal downtime. You may have mild soreness at the injection site for 24-48 hours. Pain relief typically begins within days to weeks, depending on the injectable used. Post-injection physical therapy integration is crucial, gentle movement and structured rehabilitation help maximize results and restore mobility. Avoid strenuous activity for 48 hours; your clinician will provide a personalized recovery timeline and guidance on when to resume normal activities and exercise.
This article was written using GrandRanker